



A Look at Chromosomes and Genes
We’ll start here with some background on chromosomes and genes. You can also refer to our list of definitions.
Chromosomes
Our bodies are made up of about 60 trillion cells. There are more than 200 different types of cells, each of which manufactures proteins. The kinds of proteins any given cell makes determine its particular characteristics, which in turn create the characteristics of the entire body. Bones, muscles, blood, and hair, for example, are all made up of proteins.
The instructions for making these proteins are stored in molecules called DNA. Chromosomes, which are found in the center, or nucleus, of all of our cells, including egg and sperm cells, serve as the structure that holds the DNA.
Chromosomes are passed down from generation to generation through the egg and sperm. Typically, we all have 46 chromosomes in our cells, two of which are sex chromosomes. Females have two X chromosomes (XX) and males have one X chromosome and one Y chromosome (XY).

Genes
The job of a gene is to either make a protein — the building blocks of all the structures in the body — or to regulate other proteins in the body. Our bodies contains an estimated 25,000 to 35,000 genes.
DNA is the material that makes up the chromosomes and genes located in a cell’s nucleus. Genes are sections of DNA that carry the information that determines the traits passed from parents to their children, and are located on the (typically) 46 chromosomes in each cell.
DNA needs to be in a certain pattern or order, like the numbers in a phone number. The pattern of DNA determines if the gene is working properly.
A gene has three regions that work together like a factory or machine:
- Promoter Region: The “promoter” turns the gene on, like a light switch.
- Coding Region: The “coding region” includes the protein building information. “Introns,” also referred to as “filler,” are sections that act as placeholders in between “exons,” which are used to make a protein. Most genes have many exons separated by introns.
- Termination Sequence: The “termination sequence” designates the end of a gene.

How Does a Gene Make Proteins?
The DNA in the gene is a code that is “transcribed” (or talks) to another kind of molecule called RNA. This is like matching up one side of Velcro to the other (hook side and loom side). The RNA then “translates” the DNA to put together the protein.
The FMR1 Gene
Genes are named as they’re discovered. Usually, the name isn’t exactly the same as the condition. This is done in case it’s later discovered that there’s more than one gene involved in the condition.
The gene that causes Fragile X is called the FMR1 gene, which now stands for Fragile X messenger ribonucleoprotein 1. At the time of discovery, it stood for Fragile X mental retardation gene, and “mental retardation” was the accepted term for what we now refer to as “intellectual disability.” Today, we simply refer to it as the “FMR1 gene” or the “Fragile X gene.”
The FMR1 gene is located on the X chromosome. We all have 46 chromosomes — 23 pairs — in each of our cells. The first 44 — 22 pairs — are numbered 1 through 22. The last two — pair 23 — are the sex chromosomes.
Females have two X chromosomes (XX) and males have one X and one Y chromosome (XY).
There are many genes on each chromosome. Like houses on a street, each gene is given an address, depending on where it lies on the chromosome. The address of the FMR1 gene is Xq27.3.
 Credit: Chromosome karyotype, Zappy’s Technology Solutions.
Credit: Chromosome karyotype, Zappy’s Technology Solutions.
Does everyone have an FMR1 gene?
Yes, everyone has an FMR1 gene. When someone states, “I have the gene for Fragile X,” they really mean they have a gene mutation for Fragile X. Some Fragile X genes are normal and some are not.
Learn more about the “Normal Function” of the FMR1 gene from the CDC.
What does the FMR1 gene do?
The FMR1 gene makes a very important protein called FMRP (Fragile X protein). Though this protein is found in all our cells, it’s most abundant in the nerve cells, and particularly in a part of the nerve cell that “talks” to other nerve cells called “dendrites.”
How does an FMR1 gene mutation cause Fragile X syndrome?
A mutation is any change in a gene. Some mutations don’t cause any problems and we don’t know about them (unless found in the laboratory). Mutations in the FMR1 gene involve an abnormal expansion of the DNA in the promoter region of the gene.

Often a mutation causes decreased or absent protein production. In individuals with a “full mutation,” their FMR1 gene is shut down and they don’t make enough or any FMRP.
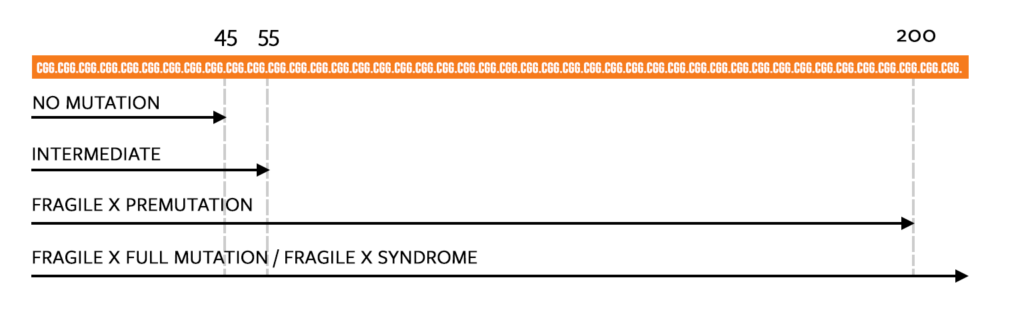
CGG Repeats: The Four Forms of the FMR1 Gene
The FMR1 gene appears in four forms that are defined by the number of repeats of a pattern of DNA called CGG repeats.
DNA is made of molecules that are abbreviated A, C, G, and T. A CGG repeat in the FMR1 gene is a pattern of DNA that may repeat itself anywhere from 30 to 1,000 times. In the FMR1 gene there is an area of the promoter region that is rich in these CGG repeats and is measured when Fragile X testing is performed.
- Typical
<45 CGG Repeats - Intermediate
45–54 CGG Repeats
Those with 45-54 CGG repeats have what is called an “intermediate” or “gray zone allele,” which does not cause any of the known Fragile X associated disorders. - Premutation
55–200 CGG Repeats
Individuals with a premutation carry an unstable mutation of the gene that can expand in future generations and thus cause Fragile X syndrome in their children or grandchildren. Individuals with a premutation can also develop FXTAS, which stands for Fragile X-associated tremor/ataxia syndrome (more common in males over 50) or FXPOI, which stands for Fragile X-associated primary ovarian insufficiency. - Full Mutation
200 or more CGG Repeats
A full mutation of the FMR1 gene causes Fragile X syndrome.
The full mutation causes the FMR1 gene to shut down or “methylate” in one region. Methylation happens to other genes when they’re supposed to be turned off (as in the genes we don’t use, like those that make a tail grow!).
Because the FMR1 gene produces the important protein called FMRP, when the gene is turned off it does not make this protein. In Fragile X the methylation turns off the FMR1 gene, so no FMRP is produced.
The lack of this specific protein is what causes Fragile X syndrome.
AGG Interruptions
When we hear a number like a 400 (a full mutation) or an 80 (a premutation) and that’s it, is that all there is to it? Just a number? We may envision a long tract of CGGCGGCGGCGG over and over again, as the genetic counselor or doctor described. But how are “AGG interruptions” related to Fragile X inheritance?
Webinar: The Genetics of Fragile X Associated Disorders
Jayne Dixon Weber hosts as Brenda Finucane, a licensed genetic counselor and professor at Geisinger’s Autism & Developmental Medicine Institute, answers your most frequently asked questions related to Fragile X and the complex inheritance pattern of the FMR1 gene.
Following the original live webinar, we heard from the community who told us how great this presentation was, and many told us it’s the best description of Fragile X that they’ve ever seen.
Please note that you can use the chapters tool at the bottom right of the video screen to find specific sections of the video, including reproductive options, FMR1 expansions, and mosaicism.
Inheritance: Premutation and Full Mutation
Fragile X is an “X-linked” condition, which means the FMR1 gene is on the X chromosome.
In most X-linked conditions, all males who carry the abnormal form of the gene are affected. Fragile X syndrome is unique in that unaffected males can carry the gene in the premutation form while themselves having no symptoms of the condition.
Most X-linked conditions are also not passed on to daughters. Fragile X syndrome is unique here too, because it can also affect females, though usually less severely than males. Because females have two X chromosomes, when they receive one X chromosome that carries a mutation, their second, “normal” X chromosome often masks its effect.
De Novo Fragile X
There are rare cases of de novo Fragile X syndrome, meaning FXS spontaneously occurred and was not hereditary.
How the Fragile X Premutation or Full Mutation is Passed on to Sons and Daughters
As shown in the video and image above:
- When a mother passes on a premutation, it’s often a larger version of the mutation, in other words, a full mutation.
- If a mother passes on a full mutation, it will remain a full mutation.
- When a father passes a premutation on to his daughters, it remains a premutation, and does not expand to a full mutation.
- In most women with a mutation, it only appears in one of her X chromosomes, which means her second X chromosome is normal. Thus, she has a 50% chance of passing on either her normal X chromosome or her mutation (premutation of full mutation) in each pregnancy.
- Because fathers who carry the premutation have only one X chromosome, they will pass it on to all of their daughters
- Because fathers only pass their Y chromosome to their sons, fathers with the premutation will not pass it on to their sons.
The Fragile X Premutation
55–200 CGG Repeats
Approximately 1 in 151 females and 1 in 468 males carry the FMR1 premutation. They are known as “premutation carriers,” often shortened to “premutations.” Premutations are defined as having 55–200 CGG repeats and can occur in both males and females. (Also see: What Defines a “Carrier”)
A common feature of premutations is that the gene can change sizes over generations, potentially expanding to a full mutation in subsequent generations.
The chance of the premutation expanding to a full mutation is related to the size of the mother’s premutation — the larger the mother’s CGG repeat number, the higher the chance that it will expand to a full mutation if passed on.
Typically, the premutation has no immediate and observable impact on a person’s appearance or health. However, some females with a premutation will experience Fragile X-associated primary ovarian insufficiency (FXPOI), which causes infertility, irregular or missed menstrual cycles, or early menopause.
Additionally, some older adults with a premutation may develop a neurological condition called Fragile X-associated tremor/ataxia syndrome (FXTAS), an adult onset neurodegenerative disorder. This is most common in males over 50.
FXTAS and FXPOI are part of the family of conditions called Fragile X-associated disorders. Fragile X-associated disorders are a group of conditions called trinucleotide repeat disorders.
The Fragile X Full Mutation
> 200 CGG Repeats
Most full mutation CGG expansions have some degree of methylation (the process that “turns off” the gene). Males with a full mutation will have Fragile X syndrome, though with varying degrees of severity.
About 65%-70% of females with a full mutation will exhibit some difficulties with cognitive, learning, behavioral, or social functioning, and may also have some of the physical features of Fragile X syndrome (such as large ears or a long face).
The remaining 30%-35% are at risk to develop mental health issues such as anxiety or depression, or they may have no observable effects of the full mutation.
Also see: The Unique Challenges for Females with Fragile X Syndrome
Definitions
Chromosome
A threadlike structure of nucleic acids and protein found in the nucleus of most living cells, carrying genetic information in the form of genes.
DNA (deoxyribonucleic acid)
A self-replicating material that is present in nearly all living organisms as the main constituent of chromosomes. It is the carrier of genetic information.
Exon
A segment of a DNA or RNA molecule containing information coding for a protein or peptide sequence.
Gene
In informal use: A unit of heredity that is transferred from a parent to offspring and is held to determine some characteristic of the offspring.
Intron
A segment of a DNA or RNA molecule which does not code for proteins and interrupts the sequence of genes.
Nucleus
The positively charged central core of an atom, consisting of protons and neutrons and containing nearly all its mass.
Proteins
The kinds of proteins any given cell makes determine its particular characteristics, which in turn create the characteristics of the entire body. Bones, muscles, blood, and hair, for example, are all made up of proteins.
RNA (ribonucleic acid)
A nucleic acid present in all living cells. Its principal role is to act as a messenger carrying instructions from DNA for controlling the synthesis of proteins, although in some viruses RNA rather than DNA carries the genetic information.
Traits
A distinguishing quality or characteristic, typically one belonging to a person.
X Chromosome
In humans and other mammals: A sex chromosome, two of which are normally present in female cells (designated XX) and only one in male cells (designated XY).
Y Chromosome
In humans and other mammals: A sex chromosome which is normally present only in male cells, which are designated XY.