Terminology: The terminology used to describe Fragile X-associated tremor/ataxia syndrome (FXTAS) can be complex and difficult to understand. Therefore, the authors of this document have attempted, wherever possible, to use everyday language. In addition, a glossary is provided at the end.
Note: A technical treatment paper for clinicians has been submitted to a neurology journal by Dr. Deborah Hall. Once published, a link will be added to the family-friendly paper. Her document will include a discussion of the medications clinicians use, based on case reports.
Introduction
FXTAS is a late-onset genetic neurodegenerative condition occurring over the age of 50 in some individuals carrying the premutation in the FMR1 gene. This gene is linked to one of the two sex (X) chromosomes. For those who do develop the condition, development and symptoms are influenced by the carrier’s CGG repeat size, sex, and age. Symptoms of FXTAS can include tremors, balance problems (ataxia), and other neurological degenerative symptoms. The condition was discovered in 2001 after clinicians noted a pattern of neurological symptoms present in parents and grandparents of persons with Fragile X syndrome.
Premutation carriers have between 55 and 200 CGG repeats within their DNA. A higher number of repeats within this range increases the risk of developing FXTAS. The CGG repeat is a normal part of our DNA. However, if the repeat becomes too long, it can stop the gene from working the way it should. Approximately 1 in 150-300 women and 1 in 400-850 men in the general population fall into this premutation carrier category.
Among premutation carriers older than 50 years, about 40% of men and 8%-16% of women develop FXTAS. This smaller percentage of affected women results from the protective effect of their second X chromosome. As a result, women have a much lower prevalence and, on average, less severe FXTAS symptoms than men, who are more frequently and more severely affected.
Learn more about Fragile X, including all associated conditions.
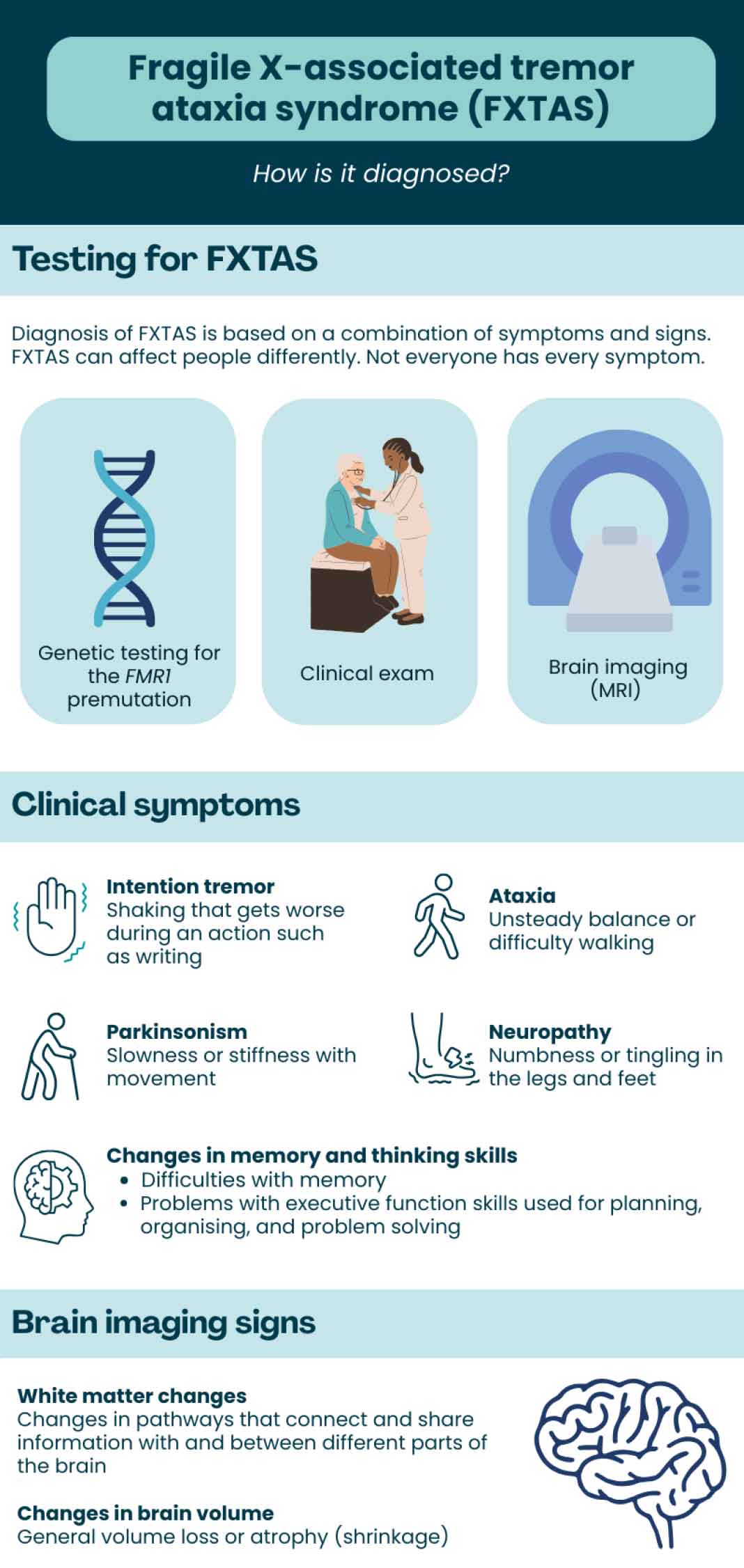
Diagnosis and Recognition
Symptoms of FXTAS vary among individuals. Signs can include intention tremor (tremor that occurs during purposeful, voluntary movement), ataxia (poor muscle control and balance), Parkinsonism, and cognitive decline, with specific impairments in executive functioning (mental processes that support goal-directed behavior by regulating thoughts and actions through cognitive control) and memory problems. (For example, forgetting what was just said in a conversation, trouble following multi-step instructions, and forgetting to take medications).
Additionally, other symptoms, such as autonomic dysfunction (problems with blood pressure, circulation, bladder and bowel control) and peripheral neuropathies (numbness or tingling in the legs and feet), may be present or develop later.
The first neurological signs of FXTAS vary for each individual. Tremor is the symptom that often leads to evaluation by a health provider. Action tremor, often referred to as “intention tremor” (during voluntary movements such as reaching for an object), is most common. Mild, intermittent tremor may be present for years before diagnosis. Tremor while at rest is less common but can also be present.
Almost all affected individuals with FXTAS develop gait ataxia as FXTAS progresses. People may have trouble maintaining balance during tandem gait (heel-to-toe walking), and unexplained falls occur in up to 50% of premutation-carrier men and in some women. Other impairments, including Parkinsonism, sensory neuropathy (tingling or numbness), and weakness, contribute to the balance problems associated with FXTAS.
Although many affected patients have features of “classic” FXTAS (meaning tremor and ataxia), other neurological presentations, such as atypical Parkinsonism (such as shuffling gait, resting tremor, or difficulty in initiating movements), primary dementia, or neuromuscular abnormalities, such as progressive muscle weakness, atrophy, fatigue, spasms, or pain, can also occur.
Changes in cognitive function may impact intellectual abilities, including working (active) memory, short-term memory, and information processing. Problems with executive function may lead to psychiatric and behavioral conditions such as increased anxiety, irritability, agitation, hostility, obsessive-compulsiveness, apathy, and depression. It is important to be aware that these psychiatric and behavioral conditions can exist unrelated to FXTAS but still be related to the premutation or can be completely unrelated to Fragile X.
Individuals experiencing any of these symptoms are encouraged to include a Fragile X-knowledgeable mental health professional as part of their care team. If a Fragile X- knowledgeable professional can’t be found, a mental health provider who is knowledgeable or experienced in neurological conditions should be sought.
Lastly, individuals with FXTAS usually have specific changes in brain magnetic resonance imaging (MRI). It is important to note that our brains change as we age, and many findings on MRI, including “white matter changes,” could be from changes other than FXTAS. On occasion, an individual with the Fragile X premutation may have changes to the brain that show up on an MRI scan that are indicative of FXTAS, but not enough to make a diagnosis of FXTAS at the time of evaluation. You may hear this referred to as “prodromal FXTAS.” While these individuals may later develop tremor and ataxia symptoms and receive a diagnosis of FXTAS, the presence of changes within the brain does not necessarily indicate that the clinical condition of FXTAS will develop.”
Of note, about 20% of women with the FMR1 premutation develop Fragile X-associated primary ovarian insufficiency (FXPOI). Women with FXPOI do not have an increased risk of FXTAS compared with women who carry the premutation and have typical ovarian function. In addition, symptoms and signs of classic FXTAS have been reported in FMR1 gray-zone carriers (41-54 CGG repeats) and in those with a full mutation that is unmethylated or mosaic with a large number of cells with the premutation. However, FXTAS in people with repeat sizes outside of the premutation range is rare.
Some doctors or clinicians may refer to “FXTAS stages”; however, it is important to note that these descriptions are general and may not apply to everyone.
FXTAS Stages
- Stage 1: Subtle or questionable signs
- Stage 2: Minor, but clear, tremor and/or balance problems
- Stage 3: Moderate balance and/or tremor problems and at least occasional falls with significant interferences with activities of daily living
- Stage 4: Severe tremor or balance problems. Use of a cane or walker.
- Stage 5: Use of a wheelchair on a daily basis
- Stage 6: Bedridden
In addition, the FXTAS Rating Scale (FXTAS-RS) was developed by Dr. Deborah Hall and her colleagues at Rush University. It is a standardized neurological assessment of motor function that covers many of the key movement problems in FXTAS. For the assessment, the patient is asked to do a series of tasks involving the arms and hands (writing, pouring water, reaching), walking, and balance, and the trained clinician carefully observes and records the severity of several neurological issues such as tremors, atypical eye movements, balance while walking and standing, and the speed and quality of movement.
Current Treatment Recommendations
Treatments for FXTAS must be individualized because symptoms vary from person to person. Symptom management is often similar to that utilized for treating Parkinson’s disease. The goal of therapy for FXTAS is to reduce symptoms and slow its progression. Treatments should also be approached globally, using multimodality interventions, including medications, psychological counseling, and rehabilitative interventions such as speech, occupational, and physical therapy, as well as gait training. Consideration should also be given to supportive services and counseling for the family.
Specialty fields helpful in the care of individuals with FXTAS include neurology and movement disorders neurology and often include psychiatry, psychology, rehabilitation, urology, cardiology, speech & language pathology, physical therapy, occupational therapy, and audiology.
Management of FXTAS can be complex and involves appropriate follow-up by an adult neurologist. It is also important to evaluate other potential causes of memory and cognitive problems, such as vitamin B12 and folate deficiencies, as well as depression.
Treatable causes of ataxia should be considered in cases when there are significant gait symptoms. This typically includes testing liver and renal function, Vitamin E, Copper, thyroid function, autoimmune issues (SSA/SSB, ANA, Gad-65, Celiac), and paraneoplastic disorders. (Where the immune system, while fighting a cancer, mistakenly attacks healthy body tissues.) Reversible causes of neuropathy should also be considered, including diabetes, monoclonal proteins, vitamin B12 deficiency, and folate deficiency. Additionally, individualized evaluation regarding possible adverse events from medications is essential.
Referral to physical therapy or rehabilitative medicine, urology, genetic counseling, and social work should be considered. Preventing falls should be emphasized, including the use of assistive devices such as canes or walkers. Other medical issues to be evaluated and treated as necessary include hypertension, sleep apnea, and hypothyroidism. Lastly, the importance of good nutrition and regular exercise cannot be overstated and is strongly recommended by those providing FXTAS treatment.
—Medications
As of 2026, there are a small number of studies looking at medications for FXTAS. Since FXTAS can affect people in different ways, treatment is usually individualized based on specific symptoms rather than a one-size-fits-all approach. Past research shows that a variety of medication types and therapies may be helpful for some individuals with FXTAS, depending on their needs. However, it should be noted that all available medications at this time are for symptomatic relief and do not change the course or progression of the disease.
Researchers are actively preparing for future clinical trials in FXTAS, with the goal of expanding treatment options over time. While this work is ongoing, families and caregivers who want a more detailed discussion of medication can refer to a technical guidelines paper expected in the second half of 2026. Patients may also want to share the PDF version of this FXTAS article and the planned technical document with their doctor and other treatment specialists.
—Psychotherapy
Psychotherapy may be beneficial for individuals with FXTAS, particularly for the management of depression, anxiety, apathy, obsessive-compulsiveness, and difficulties adjusting to a chronic neurodegenerative condition. Structured approaches such as Cognitive Behavioral Therapy (CBT) may help patients identify and modify maladaptive thought patterns, improve coping strategies, and enhance emotional regulation.
Psychotherapy may also support stress management, reduce caregiver burden, and address behavioral symptoms associated with cognitive decline, thereby improving overall quality of life for both patients and their families. In addition, in some instances, family therapy to support the family system may be appropriate.
—Genetic Counseling
Genetic counseling for individuals with FXTAS and their family members is recommended due to FMR1 inheritance. Men with the FMR1 premutation (55-200 CGG repeats) pass it on to all of their daughters, as the gene is on the X chromosome. Women with the premutation have a 50% chance of passing it to each of their children (boys or girls). However, the CGG repeats can expand when coming from the mother. If the expansion results in >200 CGG repeats, the child will have Fragile X syndrome. Fragile X syndrome is the most common inherited form of intellectual and developmental disabilities and is the most common known single gene cause of autism spectrum disorder (ASD).
—Surgery
The use of isoflurane for general anesthesia should be avoided. If medically necessary, the anesthesiologist and primary neurologist should be consulted prior to surgery. Deep brain stimulator surgery can be considered for tremor. Unilateral surgery (one-sided) may be less likely to worsen ataxia. Note that this surgery is not common in FXTAS and comes with its own potential risks and benefits. If tremor is severe and not controlled with medication, this is something that should be discussed with a movement disorders neurologist.
Finding a Physician Knowledgeable About FXTAS
Fragile X clinics can provide information or referral to a neurologist or other physician with experience in caring for patients with FXTAS. We have a list of FXTAS clinics, including those affiliated with the National Ataxia Foundation and knowledgeable about FXTAS (800-688-8765).
Additional Resources & Glossary
- NICHD FXTAS Treatment Info
- National Ataxia Foundation FXTAS Page
- International Parkinson and Movement Disorders Society — Find a specialist
- Participate in Research — Find a FXTAS study or trial
- Learn more about FXTAS — From our blog
- Watch a FXTAS webinar — From our webinar library
Glossary
Ataxia: Loss of control or incoordination of body movements
- Cerebellar ataxia: A loss of body control caused by differences in the cerebellum, the part of the brain that coordinates movement. The first signs that someone has cerebellar ataxia might be bad balance and walking, and uncoordinated eye movements. It can cause poor articulation when speaking or slurred speech, which is called dysarthria.
- Appendicular ataxia: A form of cerebellar ataxia that lowers coordination mostly in the arms, hands, legs, and feet
Autonomic dysfunction: Changes to the autonomic nervous system. The autonomic nervous system controls things like heart rate, body temperature, breathing rate, and sensation or feeling. Dysfunction or changes in the autonomic nervous system can lead to very high or low heart rates, sweating too much or too little, weakness, and other symptoms.
Cerebellar dysarthric “scanning” speech: Words are broken into separate syllables, often with a pause between the syllables, and with each syllable spoken at different volumes.
Executive functioning: Executive functioning is an umbrella term for the skills requiring mental control and self-regulation. Executive functioning skills include inhibition (the ability to stop your behavior at the appropriate time), the ability to shift easily from one situation to another, the ability to regulate your emotional responses, and others. Impairment in executive function occurs when a person has difficulties with one or more of the executive function skills.
FMR1: Fragile X messenger ribonucleoprotein 1. Learn more about FMR1 proteins.
Mosaic: Having both premutation and full mutation repeat expansions in the FMR1 gene.
Methylation (methylated / unmethylated): Having more than 200 CGG repeats sets in motion methylation of part of the FMR1 gene. Methylation prevents the synthesis of FMRP, and its absence causes Fragile X syndrome. In FXTAS, the FMR1 gene is unmethylated, leading to elevated levels of FMR1 mRNA containing expanded CGG repeats. Learn more about methylation.
Neurodegenerative: Gradual loss and eventually death of nerve cells (neurons) in the brain or nervous system.
Neuromuscular abnormality: a broad term for diseases affecting the nerves that control voluntary muscles, the muscles themselves, or the neuromuscular junction (connection point). These conditions disrupt communication between the nervous system and muscles, leading to progressive muscle weakness, atrophy, fatigue, spasms, or pain.
Oculomotor: Having to do with eye movement
Parkinsonism: A combination of symptoms including tremor, slow movements, rigidity or muscles being tensed, and unsteadiness
Peripheral neuropathy: Caused by damage to the peripheral nerves, which are the nerves that send information from your brain and spinal cord to the rest of your body. This often feels like stabbing, burning, or tingling, especially in the hands and feet.
Sensory neuropathy: Caused by damage to the sensory nerves (these are the nerves that sense pain or temperature). It may feel similar to peripheral neuropathy, and people may also have reduced ability to sense pain or very hot or cold temperatures.
Tandem gait: Often done as part of a neurologic examination, or during an exam with a Neurologist. Walking so that with each step, the toes of the back foot touch the heels of the front foot.
Temporal sequencing: A sequence of events happening in a period of time. Remembering the order of events is important to our everyday lives.
Tremor: A quivering or shaking movement that happens when you are not trying to do it (involuntary). Action tremor occurs when you’re actively trying to do something. Rest tremor occurs when the muscles are at rest, and you are not trying to move.
FXTAS Webinars
February 9, 2026
00 h 19 m
Dr. David Hessl joined the NFXF to discuss the exciting new ACT for FXTAS study, funded by the National Institute of Neurological Disorders and Stroke (NINDS).
January 8, 2026
00 h 01 m
Descubre qué es la premutación del síndrome del cromosoma X frágil en tan solo 90 segundos.
July 29, 2025
00 h 02 m
The NFXF is excited to share the second video in our animated series designed to raise awareness and educate about Fragile X!
FXTAS Articles