This summary was extracted in part from the Autism Spectrum Disorder in Fragile X Syndrome treatment recommendation and from the original text by Dr. Dejan Budimirovic of the Kennedy-Krieger Institute FX Clinic in Baltimore.
Overlaps and Gaps Between the Two Conditions
Families and some providers are often confused by the relationship between Fragile X syndrome (FXS) and autism. It is important to note that it is more common for a child to be diagnosed with autism and then to receive an additional diagnosis of FXS.
Understanding these distinctions can be particularly helpful when deciding on the most appropriate medical, therapeutic, counseling, and education interventions, and will increase the potential for both short- and long-term benefits.
Learn more and join individuals with the premutation and their families to help advance — and encourage — deeper understanding and research into the premutation condition.
The Relationship Between Autism and FXS
Autism is a developmental disorder primarily characterized by a selective impairment in social interaction. Namely, people with autism have differences in how they understand and react to people and social situations, which result from differences in how their brains process socially relevant information.
Symptoms of autism appear in early childhood. It is a lifelong disorder, though symptoms change over time. At this time, there is no medical test, such as a blood test or brain scan, that can diagnose autism. Yet in some cases the cause of autism is known, such as Fragile X syndrome — the most common-known single-gene disorder that accounts for about 2% to 3% of all autism cases.
Specifically, FXS is a genetically defined condition that can be diagnosed by a DNA blood test, unlike autism, which is behaviorally defined. Thus FXS is one cause out of many, for a person to manifest the clinical symptoms that define autism.
Why Autistic Features Are Common in FXS
Our current autism knowledge indicates that it is a developmental brain disorder, beginning shortly after birth or even earlier. Its most characteristic feature is the presence of abnormal patterns of neural “wiring,” or connectivity. Because multiple genetic and environmental factors have been linked to autism, there are probably multiple ways in which neural connectivity and other processes can be disrupted, leading to a common outcome or set of clinical features that result in a diagnosis of autism.
In regard to the neural connectivity, many proteins that have similar jobs as FMRP (the protein made from the Fragile X gene, FMR1, which is absent or reduced in people with FXS) and also proteins that interact with FMRP have been found to be associated with autism. Thus, it is likely that autism is frequently present in FXS because the lack of FMRP in FXS adds to the risk of developing the types of abnormal wiring and related brain abnormalities that lead to autism symptoms.
FXS as Part of the Autism Cloud
It may be useful to see autism as a cloud that represents a final common diagnostic category, illustrative of abnormal patterns of brain wiring resulting from a blend of multiple diverse genetic and other etiologies.
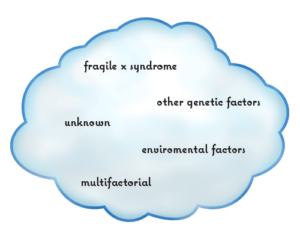 The cloud contains a common set of behavioral characteristics that are core features of autism. Individuals with FXS who meet criteria for the current definition of autism represent a spot in the cloud where one may meet criteria for ASD, but also tend to have an FXS-related type of autism with higher rates of social anxiety, intellectual disabilities, hyperarousal, repetitive behaviors, and other FXS-related differences, than those with ASD of an unknown cause.
The cloud contains a common set of behavioral characteristics that are core features of autism. Individuals with FXS who meet criteria for the current definition of autism represent a spot in the cloud where one may meet criteria for ASD, but also tend to have an FXS-related type of autism with higher rates of social anxiety, intellectual disabilities, hyperarousal, repetitive behaviors, and other FXS-related differences, than those with ASD of an unknown cause.
Yet, sometimes it is unclear whether or not someone should receive a diagnosis of autism. The level of overlap between the FXS behavioral phenotype (symptoms) and autism determines whether a person with FXS makes it into the ASD cloud. Some individuals may have enough autism features to be near the cloud, but not at the threshold needed for an actual diagnosis. Those with FXS who are in the autism cloud likely have genetic factors that add to FMRP deficiency, which pushes them toward meeting autism criteria.
Treatment Recommendations for Individuals with FXS Who Meet the Criteria for Autism
Challenging behaviors such as attention problems, disruptive behavior, anxiety, and aggressive and self-injurious behaviors, can significantly impact an individual’s academic and adaptive functioning, limiting their participation in the community.
In addition to behavioral therapy (the mainstay of treatment), medication can sometimes be helpful to support therapeutic services and to allow a child to learn in the least restrictive environment. For children with FXS, regardless of whether they meet criteria for autism, interventions that target communication and socialization skills are appropriate. However, the crucial point for teachers, therapists, and others involved in the support of individuals with FXS, is to utilize existing knowledge of behavior and learning styles typical of FXS in an individualized manner (i.e., in FXS we would not force eye contact, different from the applied behavioral analysis-based treatment of individuals with autism of unknown cause).
This approach will help to better customize educational, behavioral, and other strategies to the needs of each individual. Further molecular, educational, behavioral, and non-pharmacological therapeutic intervention studies are needed to refine our understanding of the similarities and differences between individuals with only FXS and individuals with FXS and autism. Clinical trials of both standard pharmaceutical medications and promising new treatments targeted to underlying brain mechanisms are also needed to explore whether individuals with FXS who meet or do not meet the criteria for autism respond differently to treatment.
Overall, the future not only holds hope but also the realistic potential for meaningful clinical and functional progress in individuals with FXS and autism.